VIDEO DU GLAUCOME
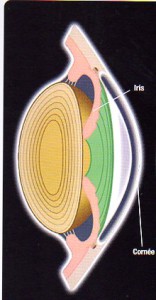
- Angle ouvert le plus fréquent
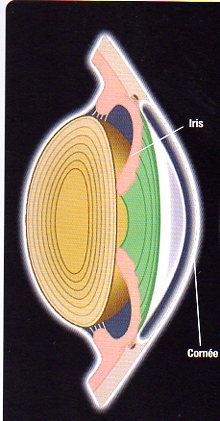
- Angle fermé moins fréquent
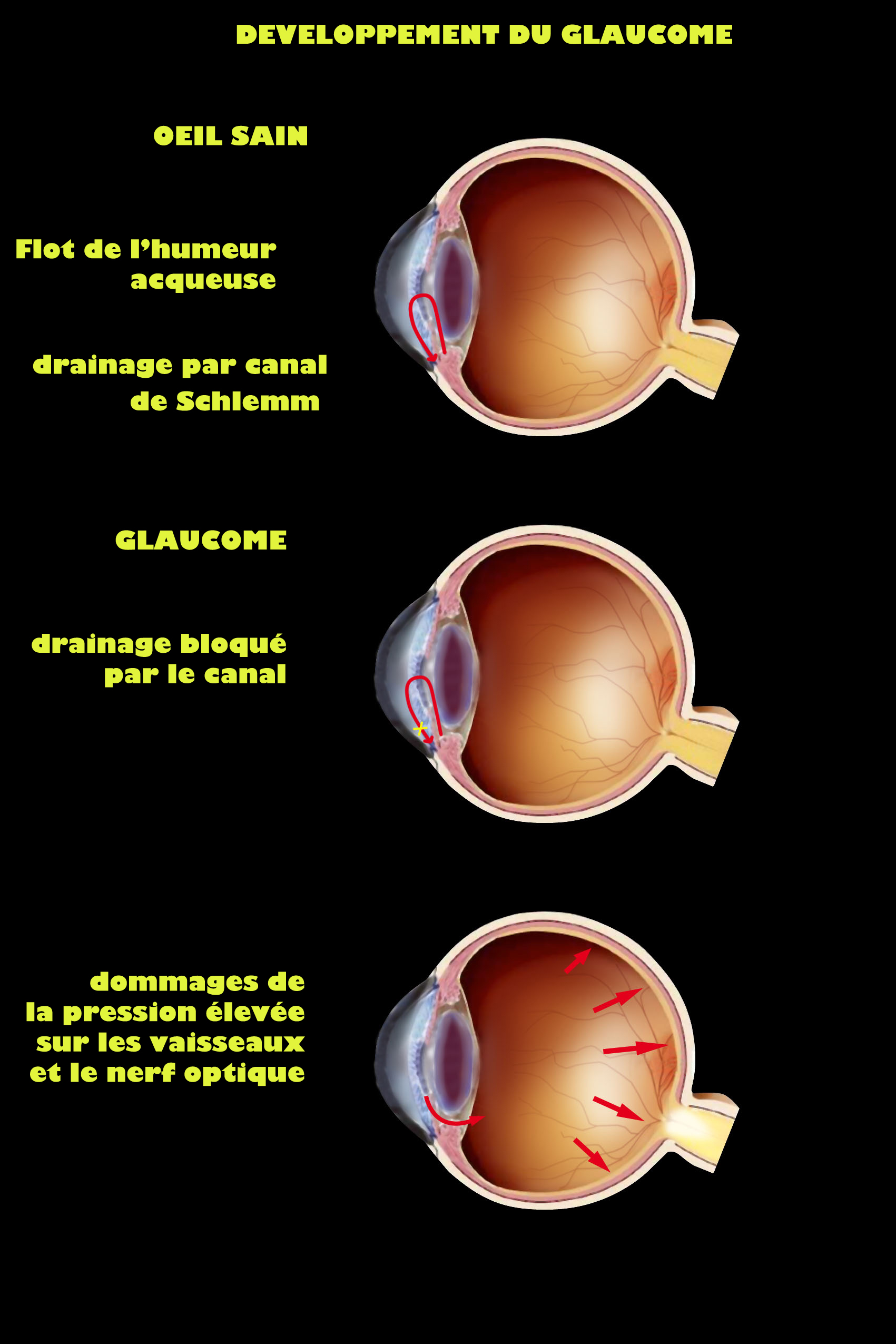
The glaucoma is due to an increase of the internal pressure of the eye. It can show himself in a acute way and realize an ophthalmologic urgency(emergency), or establish(constitute) in a slow and progressive way. It evolves, in both cases, towards the blindness in absence of treatment. So it deserves to be better known.
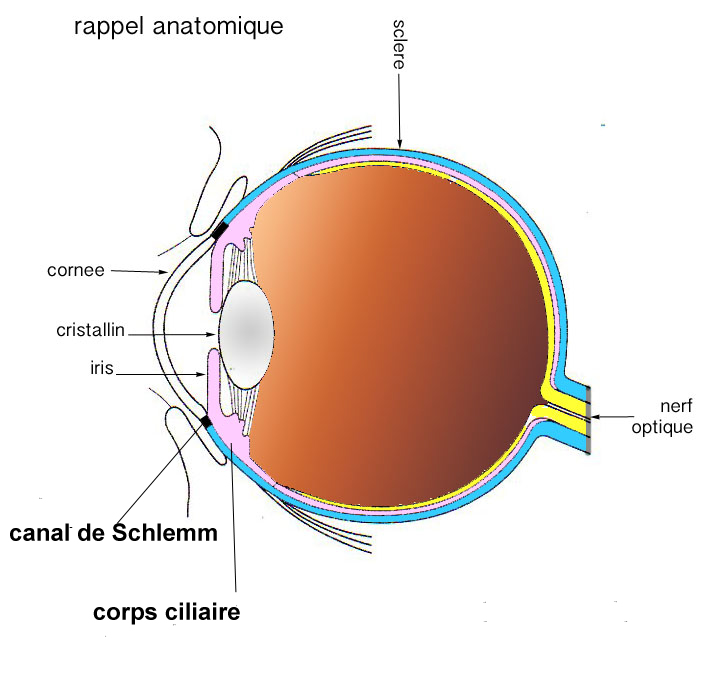
This internal pressure of the eye has nothing to do with the blood pressure. it is due to the production, inside the eye, inside the liquid called aqueous humor, which feeds the lens and the cornea, then it evacuates except the eye towards the blood circulation.
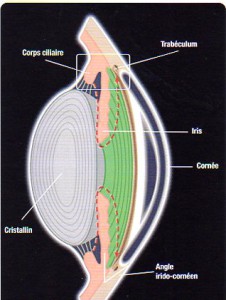
In the case of a glaucoma, it does not manage to go out easily and accumulates inside the eye, so creating a pressure interns in the eye. It evacuates by the part of the eye situated between the cornea forward, and the iris behind, called angle of anterior chamber. As this angle is wide or narrow, it establishes(constitutes) two sorts of glaucoma:
– The glaucoma chronicles in opened angle
– Or the acute glaucoma
The normal intraocular pressure is lower than 20 mm of mercury, mostly situated between 14 and 18.
The glaucoma chronicles in opened angle: the most frequent (80 % of the cases).
It shows itself mostly by an eye pain, headaches, eye redness, whimpering, burns, but very often it gives no sign and the discovery of the hypertonia of the eye is made by chance during an examination at the ophtalmologist.
The discovery of a high pressure imposes a surveillance(monitoring) or a treatment(processing), otherwise the small vessels which irrigate the second nerve are compressed, choked(repressed), where from suffering(distress) of the fibers which compose the second nerve, which eventually die by small packages.
Can we know if the optic nerve is already affected)?
Yes, by practising an eyeground, we can see the color of the head of the optic nerve, said optic disk, which becomes pale then grey or openly white, and we see an excavation in its surface which leave dead or missing fibers. Various imagings are capable of quantifying the loss of optical fibers: the retinal tomography of Heidelberg ( HRT), the tomography in optical coherence ( OCT), the analyzer of nerve fibers ( GDX).
Yes, by practising a visual field. The consequence of these missing fibers is translated in the visual field by a lack, a deficit. As it is always the same fibers of the second nerve that suffer in the first one, the deficit of the visual field at the beginning is always made in the same zone, and consequently becomes typical of the glaucoma.
The acute glaucoma: an urgency.
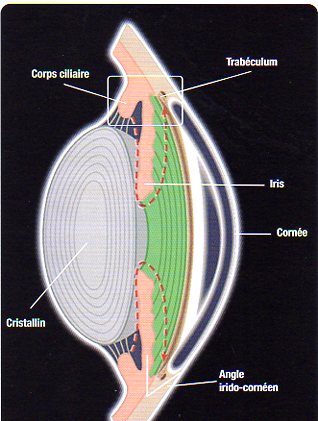
The angle of anterior chamber by which evacuates the aqueous humor is narrow and becomes it even more in certain circumstances: when the pupil dilates, in the darkness, by mydriatic collyrium or in period of stress, the iris curls up in accordion and blocks the already narrow angle.
The aqueous humor cannot evacuate any more and the pressure rises brutally where from crisis made by eye pains, ” Here stops(arrests) the translation ” of headaches, eye fog and of colored haloes. In the palpation, the eye is hard. The intraocular pressure can rise to more than 40 mm of mercury.
An urgency is which it is necessary to treat by collyria, tablets then operation. It can have recurrences or infringement(achievement) of the other eye there.
To avoid recurrences, we practise a trabeculectomy. It is an opening which allows the aqueous humor accumulated to evacuate easily except the eye.
To avoid in the other eye the same fate(spell), we practise a preventive said operation iridectomy, practised mostly by means of the laser Argon or YAG in ambulatory or more rarely by surgical way with a local anesthesia.
TREATMENTS
By collyria, which decrease the secretion of the humor acqueuse (agonist alpha adrenergic, béta-bloquants and inhibitors of the carbonic anhydrase)
and those who facilitate its exit except the eyeball (prostaglandins, agonist alpha adrenergic and agonist adrenergic)
by laser (after failure(insufficiency) or failure(defeat) of collyria) at the level of the angle of anterior chamber, to improve the exit of the humor acqueuse
by surgery to create an exit in the acqueuse humor
by the neuroprotection: a neuroprotective drug is an agent who prevents the death of nerve cells.


